
This Article From Issue
September-October 2004
Volume 92, Number 5
DOI: 10.1511/2004.49.0
Monturiol's Dream: The Extraordinary Story of the Submarine Inventor Who Wanted to Save the World. Matthew Stewart. xiv + 338 pp. Pantheon, 2003. $25.
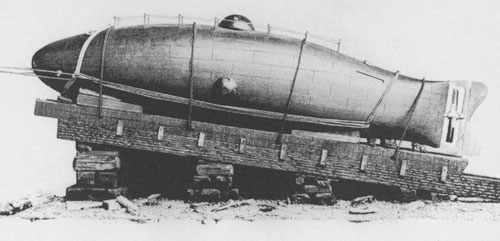
In the summer of 1859, Narcís Monturiol i Estarriol and his crew ran sea trials of the Ictíneo, the world's first fully operational submarine, in the harbor waters of Barcelona. This untethered, double–hulled, hand–powered vessel built of copper–sheathed olive–wood staves proved capable of routinely diving to 20 meters and of navigating at that depth with a crew of up to six men. Thus the Ictíneo was far superior to the pioneering submarine most Americans know about: the Hunley, which was used in the Civil War.
Monturiol, who invented the Ictíneo, was not an engineer; rather, he was an idealistic visionary. His little–known story is ably recounted by Matthew Stewart in Monturiol's Dream: The Extraordinary Story of the Submarine Inventor Who Wanted to Save the World.
In the first half of the book, Stewart describes Monturiol's remarkable life as a socialist revolutionary and a follower of the utopian thinker and influential communist Étienne Cabet, who promoted a new earthly paradise in Texas called Icaria. Monturiol was one of the leaders of a progressive movement in Barcelona that advocated the advancement of both sexes. Also, he associated with the likes of bourgeois reformist Ildefons Cerdà, a civil engineer whose innovative design for the expansion of Barcelona and treatise on urbanization laid the groundwork for modern urban planning.
How does a person who spent his younger years fighting for social justice while earning a living by painting stylish portraits end up designing a state–of–the–art submarine? Monturiol's youth was defined by rauxa, a Catalan word meaning "exalted passion." He held on to his rauxa even as he abruptly abandoned his revolutionary past and embraced seny—the common sense that built the machines and factories fueling the economy of Barcelona. This combination of rauxa and seny led Monturiol to dream of building a submarine.
Ad Right
Monturiol hoped such an invention would immediately benefit one particular group of workers—coral divers—and would eventually serve as "a prototype for efforts to improve the conditions of the landlocked workers of the world." His ultimate goal was the construction of a craft that would be capable of descending to the greatest depths of the ocean and navigating underwater indefinitely; it was to be a pacific vessel, harvesting the corals and fishes of the deepest waters and seeking to promote understanding of the nature of Earth's oceans through science and technology. He conceived of his submarine, Stewart says, as a "liberational technology, one that would spread democracy across the seas" and serve as "the pilot vessel on humankind's journey toward utopia."
Stewart describes compellingly Monturiol's inspired solutions to problems of submersible design, his initial brilliant technological successes and his fight for funding. We get taken on a roller–coaster ride through the inventor's trials, triumphs, frustrations, despair, capitulation and penury. Along the way, many personalities of 19th–century Barcelona are introduced—so many that they threaten to overwhelm Monturiol's story; readers must be vigilant to keep track of his path.
Monturiol, as he worked on his design for the Ictíneo (the name could mean either "fishlike boat" or "new fish," he said), was diligent in trying to learn from the subaquatic experiences of a number of predecessors who had tried to launch submarines. He managed to solve a number of problems that had daunted them—problems of pressure, control of buoyancy and stability, life support, underwater vision and propulsion.
For Monturiol, Stewart says, diving in the Ictíneo was "transcendental, a near–death experience." Monturiol himself described it as follows:
The silence that accompanies the dives; the gradual absence of sunlight; the great mass of water, which sight pierces with difficulty; the pallor that light gives to the faces; the lessening movement in the Ictíneo; the fish that pass before the portholes—all this contributes to the excitement of the imaginative faculties. . . . there are times when nothing can be seen outside by natural light, when one sees nothing but the obscurity of the deep; all noise and movement stops; it seems as though nature is dead, and the Ictíneo is a tomb.
Tragically, in 1862 the Ictíneo was destroyed while berthed in the Barcelona harbor, "victim to a hit–and–run attack by an irresponsible freighter." Monturiol set about building a second submarine with ardor. Practical considerations—a need to raise money to pay off debts—led him eventually to equip this second vessel, the Ictíneo II, with a cannon, which he somehow justified to himself as being "all part of a plan to achieve universal peace." This submarine proved to be too stealthy: Unannounced demonstrations of its ability to load, aim and fire the cannon underwater created loud thunderclaps and tall splashes of water in the Barcelona harbor, startling unsuspecting port authorities and arousing their wrath. Monturiol was charged with disturbing the peace. When the cannon failed to achieve its purpose of attracting support from the Spanish government, Monturiol turned to the U.S. Secretary of the Navy, offering the Ictíneo II for submarine warfare in exchange for funds; but the Civil War had just ended, and the Navy had no pressing need.
Monturiol forged ahead with "perhaps the finest of his technological achievements": the addition of a steam engine to his submarine. But he couldn't keep it underwater longer than 20 minutes without the interior overheating, and he couldn't afford to try the solutions he envisioned for keeping it cool. The association of shareholders that was backing him went bankrupt, and the most advanced submarine of its day was seized by creditors and sold to a businessman. The purchaser, on receiving a large tax bill from the government for his new possession, ordered the vessel scrapped. Its surface motor was removed to a textile factory; its viewports ended up as bathroom windows. It was an ignoble end for a remarkable machine. We are fortunate to have Stewart's remarkable book to help preserve the memory of the Ictíneo and of its inventor, Monturiol.—Cindy Lee Van Dover, Biology, College of William and Mary, Williamsburg, Virginia
American Scientist Comments and Discussion
To discuss our articles or comment on them, please share them and tag American Scientist on social media platforms. Here are links to our profiles on Twitter, Facebook, and LinkedIn.
If we re-share your post, we will moderate comments/discussion following our comments policy.