To See for One's Self
By Darin L. Wolfe
The art of autopsy has a long history and an uncertain future
The art of autopsy has a long history and an uncertain future

DOI: 10.1511/2010.84.228
On a gray November morning during my pathology internship, I stood alone in the morgue of Indiana University Hospital amid the gentle buzzing of fluorescent lights and the steady drip of a faucet into a stainless steel sink. A recently deceased woman lay on the metal table, her skin pale yellow and smooth. She still wore earrings, a wedding ring and makeup. Plastic tubes and IV lines protruded from her body—the last throes of medical intervention.

Joe McNally/Getty Images
With a sense of awe and excitement, I readied myself to perform the ancient ritual of autopsy. Although I had seen dying patients as a medical student, I had not been the lone person in a room with a dead body since dissecting a cadaver in my first year of medical school. There is the stillness of inactivity, and there is the manic stillness one experiences at these moments. Adrenaline amplified the physiologic responses of my body. I became aware of my breathing, the rushes of warm air crinkling my paper surgical mask, and the thumping of my heart as its pace increased. Although the body before me was now as unfeeling and inert as any other inanimate object in the room, I sensed the life this woman had lived, as a young wife, daughter, perhaps sister or mother, now mourned after a long battle with disease. I struggled to let go of my innate aversion to death, accept its finality, and separate the person from the body that remained.
Focusing on my task, I performed the standard external examination, the pathologist’s counterpart to the traditional physical exam a family doctor, internist or surgeon might perform. While preparing my opening cut, I found a prominent, grapefruit-sized lump where the shoulder meets the upper chest. I steadied my hand and pressed the blade against the skin, puncturing the epidermis and deep soft tissue until the scalpel hit bone. The skin retained enough elasticity to recoil from my blade, and I quickly completed the series of cuts to create a Y-shaped incision on the chest and abdomen. I examined the tissues of the chest wall, which revealed a fleshy mass of disorganized white tissue that extended from within the breast into the underlying skeletal muscle and ribs with an implacable grip.
This was the nature of cancer, perfectly illustrating the etymology of the word, from karcinos, crab. The name was coined by the great Greek physician Hippocrates, based on the tendency of infiltrative malignant tumors to spread in stellate, finger-like projections that resemble a crab’s legs and claws. The word autopsy, from the Greek meaning “to see for one’s self,” expressed my experience here, developing my understanding of malignant tumors with my own eyes, a skill I would cultivate for the remainder of my career as a pathologist. It was a humbling episode to see such a personal, flagrant and advanced display of this illness in a woman of my own age. I felt honored to be the only one to lay eyes and hands on the very substance of the disease that had brought this woman to her death. I also felt a sense of connection with the physicians of eras long past who took the leap from merely observing the surface of a body to seeing what was within. Such discovery is the purest form of medicine, when a clinical condition can be directly linked to observed physical manifestations. And although the gross and microscopic features of cancer and other diseases have likely had a similar appearance in humans over time, the ways in which we discover and interpret their causes have changed dramatically.
Autopsy has been and remains the gold standard for arriving at an unequivocal assessment of the diseases and traumas that commonly affect individuals and populations. Yet autopsy is receding as a central medical procedure. Given the ubiquitous depictions of autopsy in television crime shows, one might think that morgues are overflowing with pending cases. In fact, whereas the number of murders, suicides and accidents typically keeps the coroner and medical examiner’s office thoroughly occupied, the hospital-based pathologist has experienced a huge decline of autopsies over the past half century. The autopsy rate in the years leading up to the 1950s held steady at over 50 percent; in the years since, the autopsy rate for all hospital deaths has collapsed to a present-day estimate of approximately 6 percent. This despite the fact that autopsy findings reveal a striking error rate in premortem diagnoses, and that autopsy is in fact the main mechanism for determining that error rate. A few statistics tell the story: Autopsy will reveal a previously undiscovered major diagnosis in up to 40 percent of cases, a number that has been constant for the 60 years that such clinicopathologic correlations have been recorded. This statistic is somewhat misleading, in that cases selected for autopsy are generally those of greatest diagnostic uncertainty. However, multiple regression analysis of decades of available data, presented in several papers by Kaveh Shojania at the University of Ottawa and colleagues incorporated study period, autopsy rate, country and case mix to show that the diagnostic error rate remains a very significant medical concern. The chance that autopsy will detect a class I error, in which diagnostic error may have affected patient survival, was 10.2 percent. The probability of “major errors,” missed diagnoses that, while important, probably did not affect outcome, was 25.6 percent. It is estimated that 35,000 patients who die in United States hospitals each year might survive to discharge if these hidden conditions were discovered earlier.
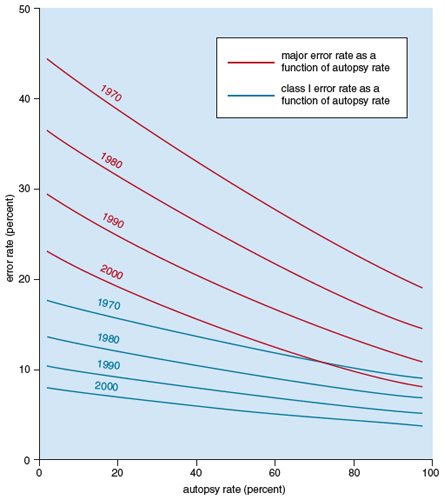
Figure adapted from Shojania, K., et al. 2002.
Diagnostic incompetence is not necessarily or even often the culprit. Some discrepancies in diagnosis between the clinic and the autopsy room must be attributed to the limits of diagnostic technology and the inevitable challenges presented by patients with multiple medical problems, atypical presentations of disease or disease that may be clinically hidden. Yet the scale of the error statistics clearly suggests the importance of the autopsy in monitoring and improving outcomes. And that is just a single benefit of the procedure. The extent of other benefits may be surprising: In addition to confirming and correcting clinical diagnoses, it is the tool for establishment of the cause of death; discovery and characterization of new and changing diseases; evaluation of new diagnostic tests, surgical techniques, devices and drugs; investigation of environmental and occupational hazards; generation of accurate vital statistics; assessment of the quality of medical practice locally and nationally; reassurance of family members about quality of care and cause of death; protection against false liability claims. Very importantly, it has tremendous value in the education of physicians and students—and most important of all, it continues to extend the boundaries of medical knowledge.
Autopsy is an old art. It has an uncertain future—and a stirring past.
Curiosity about natural phenomena has always been the fuel for scientific endeavor. One by one, great mysteries of life have been illuminated by the inquisitive mind, often going against the grain of accepted dogma. Medical science has been no exception, as demonstrated by the overlapping eras of thought that supposed, for example, demons and spirit activity as the cause of disease, even as more secular, modern explanations were emerging.
The early predominating theory of disease in ancient Greece—as well as India and Tibet—was the concept of the “four humors,” generally associated with the four elements of earth, air, fire and water, which in turn configure human personality. The theory of humors postulated that all human afflictions resulted from imbalances in these internal elements, manifest in phlegm, blood, yellow bile and black bile. For instance, an individual suffering from depression was diagnosed as having a surfeit of black bile. (The term melancholy is formed from the Greek words meaning “black” and “bile”). Likewise, a “phlegmatic” personality was associated with the more lethargic or apathetic qualities. This school of thought was prominent in the time of the great Greek physicians such as Herophilus, the first systematic anatomist; Hippocrates, whose medical canon rejected supernatural explanations of disease; and Erasistratus, follower of Herophilus and one of the last of that era—and the eon to come—to dissect human bodies.

The role of humors was articulated most eloquently by the man known as Galen of Pergamum (129–200 AD). Galen’s magnum opus on treatment, De methodo medendi, along with other tracts by him, were the first great written works of medicine and served as the universal guide to human disease for more than a millenium.During the time of Galen and of his disciples who followed, the unapproved dissection of a human body was fervently condemned. As a result, Galen based most of his understanding of human anatomy on the dissection of animals, including Barbary macaques, a type of monkey found predominantly in North Africa. Galen made the reasonable but dangerously imperfect assumption that the inner structure of such animals was close enough to that of humans to be sufficient for an understanding of human anatomy. Galen’s teachings persisted in Europe and Greece until the 16th century, and some ancient schools of medicine, such as the Ayurvedic and Tibetan traditions, still practice metaphysical healing and humor-based diagnostics that sprang from the same roots, combined with highly sophisticated pharmacology and therapeutics. Indeed, when Tibetan rulers held two major medical conferences in the 8th and 11th centuries, bringing together physicians (and translators) from India, Persia, Nepal, Greece, China and elsewhere to share their knowledge, it was Galen’s medicine they used as the basis for their integrative medical system.

Musee des Beaux-Arts, Marseille, France/The Bridgeman Art Library International
The generally accepted Galenic (humoral) approach changed dramatically in the 1530s when Andreas Vesalius, a physician and anatomist in Padua, Italy, surmised that the assumptions of Galen about the similarities between animal and human anatomy, not to mention Galen’s errors of observation, were blocking deeper understanding of the human body. Vesalius concluded that nothing less than the careful dissection of human corpses was essential for true knowledge and characterization of human disease. In 1539, a Paduan judge who shared an interest in Vesalius’ work, granted physicians the right to dissect corpses of executed criminals, thus providing the ultimate—if controversial—source of anatomical knowledge: a newly deceased human body. It is said that the accommodating judge would schedule executions for the convenience of Vesalius. The work of Vesalius was critical in expanding the breadth of medical knowledge and signaled the dawning of a new era in the science of anatomy. As the body count of executed and autopsied criminals rose, so did the cumulative anatomical knowledge of Vesalius. The investigations of Vesalius culminated in the 1543 publication De Humani Corporis Fabrica—On the Structure and Function of the Human Body. So comprehensive and detailed were his findings that Vesalius is now known as the father of human anatomy. With the publication of his work, the path to a true understanding of the inner structure and function of the human body was opened. Western medicine was transformed from a loose collection of trusted remedies and superstitions to a discipline based in logic and observation, and another area of nature previously shrouded in mystery was liberated and assimilated into the collective library of human knowledge.
The wealth of information garnered from the dissection of human corpses was cherished and nurtured, and eventually medical schools encouraged the use of cadavers in teaching. The problem was that there simply weren’t enough bodies to go around; the number of executed criminals was far less than the number of cadavers needed for medical school gross anatomy courses. As a result, corpses became highly sought after and as is often the case when something is scarce, the price was driven up and dubious enterprises were launched. Among the innovations of Vesalius himself must be counted the murky traffic in bodies ignobly acquired for a noble end. As reported in Charles O’Malley’s seminal biography of Vesalius:
Like any true scholar, Vesalius advised recourse to the sources, in this instance human bodies, and if bodies were not readily available the student was encouraged by word of mouth, or, in the Fabrica, by anecdotal precept, to seek them out for himself. It is significant that wherever Vesalius traveled to give extramural lectures a wave of body snatching ensued; the various anecdotes in the Fabrica give no indication of repentance ….
As the practices and knowledge of Vesalius became widespread, the need for cadavers resulted in the “body business,” and body snatching from graves became commonplace. Higher prices were offered for fresher bodies and body parts than for those in various states of decay. This lured some entrepreneurs into ghoulishness. Concerned families were forced to take extra precautions to protect their loved ones from the “resurrection-men,” as they were known, such as burying the bodies in reinforced coffins that were sealed shut, and hiring guards to protect the graves from desecration.

Hulton Archive/Getty Images
Many medical schools developed a “don’t ask, don’t tell” policy for students’ acquisition of human material for dissection. If a student came to class with a corpse, it was used for dissection with no questions asked. This practice again drove the demand for bodies as well as the competition among body snatchers. But while many were paying top dollar for bodies, limbs and brains taken from the grave, there were others ushering people to their deaths prematurely so that their bodies could be sold. The two most infamous of these body snatchers, William Burke and William Hare, made a short-lived career of murdering citizens and delivering still-warm bodies, saving themselves the trouble of digging up corpses from the ground while providing bodies that brought the highest price for freshness. Burke and Hare broke into the trade when a tenant of Hare’s boarding house expired from natural causes. The men carried the body to the University of Edinburgh, where they were rewarded with 7 pounds 10 shillings (roughly a thousand inflation-adjusted dollars).
Having found their buyer, they turned themselves to the problem of supply, launching a murder spree that ran to 16 victims in 12 months. Upon capture, Hare was given immunity to testify against Burke, to the rage of the populace, which was somewhat mollified when Burke was hanged—and afterward, publicly dissected.
The outcry over these body snatching practices resulted in England’s Anatomy Act of 1832, which addressed, according to the Lancet, “the system of traffic between resurrectionists and anatomists, which the executive government has so long suffered to exist.” The Anatomy Act expanded the pool of legally available corpses to include the unclaimed homeless, of whom many were easily collected from prisons and workhouses. Eventually, with the advent of the Anatomy Act and a new allowance for the donation of bodies by private citizens, the market for body snatching came to a close.
I had just completed the standard Y-shaped incision of my first autopsy when the attending pathologist entered the room, apparently unaware of my lack of experience. “Go ahead and Rokitansky the body,” he said in a serious monotone. While I had no idea who or what Rokitansky was, I guessed he was referring to the removal and examination of the internal organs. The pathologist scrutinized my every cut and guided my hands with worldly instruction. I spent more than an hour slicing soft tissue, cutting through ribs and manipulating organs this way and that with specific and directed cuts. With blood-soaked sleeves and a dampened brow, I finished the first autopsy of my career. I had “Rokitansky’d” my first body.

Getty Images
The German physician Karl von Rokitansky (1804–1878) was one of the earliest proponents of using pathological anatomy and autopsy studies to learn clinical medicine. As head of the Pathology Institute at the premiere hospital of Europe, the Allgemeines Krankenhaus in Vienna, Rokitansky is reported to have supervised more than 70,000 autopsies and performed more than 30,000 on his own—a seemingly implausible feat of labor that yet appears to be true. In his time he was widely considered the most masterful practitioner of his art. In an era when speed of dissection was key to completing an autopsy before decomposition could set in, Rokitansky invented a procedure in which the internal organs are dissected in situ and removed en bloc, thus retaining the anatomical relationships between organs. It should be noted, however, that many pathologists use the term “Rokitansky” to actually refer to the en masse technique, the procedure I used with my breast cancer patient. The en masse technique is a remarkably efficient way to eviscerate the body with a few directed cuts, allowing one to remove the organs of the neck, chest, abdomen and pelvis in one large block, with the organs retaining all of their original anatomic relations. The organ block removed from the body is completely dissected on a separate table.
The other common eponymous autopsy method is the Virchow technique, named after the German pathologist Rudolf Virchow (1821–1902), whose contributions to the field of pathology are too vast to be summarized here. In short, he is thought of by many as the first pathologist, undoubtedly most famous for his theory that disease begins first at the cellular level, a concept that was far ahead of its time. The autopsy technique that Virchow pioneered entails removing organs systematically and dissecting each organ in sequence as the autopsy proceeds. Many forensic pathologists prefer to use this technique, as it often shortens the time needed to perform an autopsy—ideal for a pathologist who has multiple bodies in the cooler awaiting postmortem examination. The anatomic relationships between organs are generally not maintained in this technique. For this reason, many pathologists employ a hybrid of both techniques, choosing to remove some organs one by one and some en bloc, particularly the heart and lungs, for which the anatomical and vascular connections may be the target of investigation for such disorders as blockages or ruptures.
One of the goals of modern medicine is to use new technology to accurately diagnose disease while minimizing the invasiveness of the diagnostic procedures. The great machine of technology has affected medicine as much as any field, producing such advances as fiber-optic endoscopes and high-resolution radiologic scanners, as well as placing more emphasis on molecular genetic solutions for preventing and treating disease.
Despite nearly 200 years of routine performance of autopsies, the procedure has changed little over time. Systematic, direct visual and tactile investigation remains the ideal. Recently, however, there have been attempts to move toward less invasive postmortem procedures that rely less on cutting and more on radiologic imaging. Not only are these techniques quicker and cleaner, they leave the body virtually undisturbed prior to work by the mortician. This offers advantages to families concerned about the body being dissected, and also to clinicians, since autopsy reports may be more quickly generated.
One method known as “biopsy-autopsy” involves sampling each organ by inserting a needle and withdrawing a small core of tissue, similar to the diagnostic biopsy used on living patients. Although this method produces very little injury to the body, it requires great skill and in many cases luck. Without the assistance of radiologic imaging such as ultrasound or computed tomography (CT), the sampling of these organs is basically a “blind” biopsy. Diseases that do not require great precision in sampling, such as large tumors or chronic liver disease, lend themselves quite well to this technique. On the other hand, a focally occurring disease such as acute myocardial infarction (heart attack) is best identified by simply holding the heart in one’s hands and slicing each of the major coronary arteries in millimeter increments, as well as slicing the heart muscle itself, in order to in order to observe obstructing clots, ruptures, or necrosis. The yield of a biopsy in this type of clinical situation would be inconsistent at best and most certainly would increase the occurrence of false negatives.
An even less invasive autopsy method is the postmortem Magnetic Resonance Image (MRI). Like conventional MRIs used for examining such things as brain tissue and knee joints, the postmortem MRI images are interpreted by a radiologist. This method does not damage the body and it produces excellent images due to the stillness of the corpse, but it cannot give a complete and trustworthy result for diseases with more subtle or absent anatomic characteristics, such as infections or electrolyte disturbances.
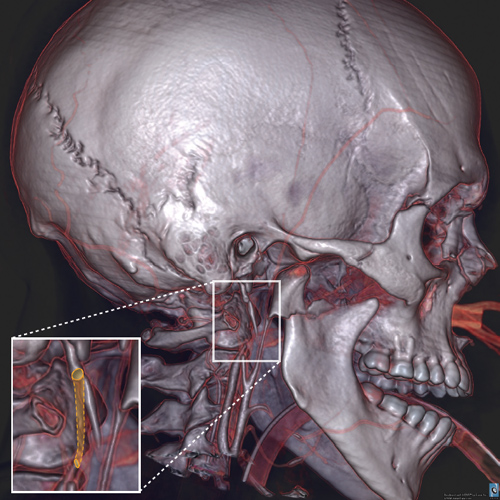
Image courtesy of Lars Christian Ebert, University of Bern Institute of Forensic Medicine, Center for Forensic Imaging and Virtopsy
Most recently, researchers in Switzerland have applied magnetic resonance and computed tomography to produce high-resolution, three- dimensional virtual autopsies of the body, or “virtopsies,” used primarily for forensic (medicolegal) applications. Pathologists can view these image reconstructions and determine bullet paths, fluid collections, broken and shattered bones, and other evidentiary features—all without cutting the body. Additional findings such as body-fluid chemistry and toxicology may be used in conjunction with the images to arrive at a diagnosis. There are many advantages to this approach, including the creation of permanent, highly detailed digital records of the anatomic evidence in the case.
The main obstacle to the widespread use of virtopsy (and other imaging-based autopsies) is its prohibitive cost. Not including the physician’s fees, the cost of equipment for virtopsy is estimated at $2–3 million, including the MRI, CT scanner and computer hardware and software. It would be difficult to justify such expense for a procedure that is not currently well reimbursed. Moreover, patients suffering from poisoning or anatomically subtle natural death are not good candidates for this procedure, meaning the capacity for traditional autopsy must still be maintained, including the costs of equipment, laboratory space and retainers for pathologists on call.
As mentioned earlier, the rate of autopsy has reached a nadir—whereas 50 years ago a majority of hospital deaths resulted in autopsy, the rate is now about 6 percent. In fact, the situation is even more extreme. The national average is bolstered by higher rates of autopsy at a small number of teaching hospitals. In nonacademic hospitals, the number of autopsies performed often hovers between few and none. Many reasons have been put forward to explain the long decline since the 1950s. On the physician’s side, reasons suggested for the decline include fear of malpractice litigation, lack of training in seeking consent from grieving families and even the ordering physician’s fear of being discredited for having missed a diagnosis. Among patients and family members, reasons include stress at the time of death, inadequate (or erroneous) information about the procedure and concerns about cost. While the decrease in autopsy rates is certainly due to an array of factors, there are a few landmark developments that have contributed most markedly to the de-emphasis of the autopsy in medical practice.
The first development occurred at the most basic level of initiation: medical education. In 1944, the requirement that medical students perform autopsies as part of their general medical education was eliminated in the U.S. As a result, a contemporary medical student’s only exposure to internal gross anatomy prior to training as a pathologist would likely be a cadaver during medical school and live patients during surgery rotations. Instead of seeing for one’s self, doctors in training were seeing little at all. Soon, an entire generation of physicians had been trained without autopsy. With no experience of autopsy as a tool in their own educations, they felt a diminished need to order the procedure when they became practicing physicians.
In the 1950s the Joint Commission for Hospital Accreditation (JCAHO) required a minimum autopsy rate of just 25 percent for teaching hospitals and 20 percent for community-based hospitals, yet the rate hovered at around 50 percent. In 1970, however, the requirement for autopsy was eliminated completely by the JCAHO, resulting in a rapid plummet to below 20 percent, followed by a steady decline all the way to 9 percent by 1994, the last year for which official statistics on autopsy rates were gathered.
It is probable that financial considerations have been the most important cause for the decrease in autopsies. Physicians and hospitals are poorly compensated for it. Medicare ceased paying directly for autopsies in 1986. In many cases, hospitals simply absorb the entire cost of performing an autopsy. The considerable time it takes to perform the procedure and the substantial paperwork required to document a single case make it easy to see why autopsy has spent the last 25 years in critical condition. Despite the decline, studies appear regularly in the medical literature documenting the enduring value of autopsy as a performance measure, a standard of accuracy for death certificates (from which national vital statistics are derived), a teaching tool and more. The tone and titles of the articles are often plaintive: “The Vanishing Nonforensic Autopsy”; “Medical Error and Outcomes Measures: Where Have All the Autopsies Gone?”
It will be true for the foreseeable future that a vast amount of information will remain hidden from even our best noninvasive technology. There is no better illustration than the case of my young breast cancer patient. While preparing my final report shortly after the autopsy, I reviewed slices of organs removed during the procedure. Although the presumed cause of death was organ failure due to end-stage metastatic breast cancer, close examination of her tissues with a light microscope revealed tiny, branching structures overwhelming nearly all of her tissues—the evidence of an invasive fungal infection, most likely due to the suppression of her immune system by chemotherapy. In the absence of an internal examination, the final diagnosis would never have been known by the clinicians; the information itself would never have been available to improve future practices and procedures.

Bill Steber/AP Images
At a watershed moment for the American health-care system, the fate of the autopsy hangs in the balance. In the past, the study of the dead was integral to the education of young physicians and pathologists. It was also the standard for measuring the quality of medical care on an individual and national scale. Can it be that our knowledge has advanced so far that we no longer need to look within ourselves? In the near future we will see whether autopsy again becomes a central tool of modern medicine or a relic of medical history’s storied past.
Click "American Scientist" to access home page
American Scientist Comments and Discussion
To discuss our articles or comment on them, please share them and tag American Scientist on social media platforms. Here are links to our profiles on Twitter, Facebook, and LinkedIn.
If we re-share your post, we will moderate comments/discussion following our comments policy.