Rethinking Adult ADHD
By Margaret Sibley
The diagnostic category for attention-deficit/hyperactivity disorder has become more inclusive, but that does not mean the condition is being overdiagnosed.
The diagnostic category for attention-deficit/hyperactivity disorder has become more inclusive, but that does not mean the condition is being overdiagnosed.

In late 2023, while taking a break at a conference in Baltimore, I shared a New York Times chart, based on detailed census records, with a colleague from the U.S. Centers for Disease Control and Prevention (CDC). The data showed a sharp rise since 2020 in Americans reporting serious difficulty remembering, concentrating, or making decisions, which are among the symptoms of attention-deficit/hyperactivity disorder (ADHD).
Moments earlier, my colleague had presented a graph with a nearly identical curve—this one tracking the steep increase in adult stimulant prescriptions since 2020. By 2023, CDC data had confirmed that a record 7.8 percent of American adults reported an ADHD diagnosis. Google searches for “ADHD” had surged, and TikTok videos tagged #ADHD had racked up more than 20 billion views. At the very most, we were experiencing an adult ADHD epidemic in the United States. At the very least, ADHD was now suddenly very fashionable to the public. Yet, a third explanation is also possible: For better or worse, the ADHD diagnostic category might be becoming more inclusive.
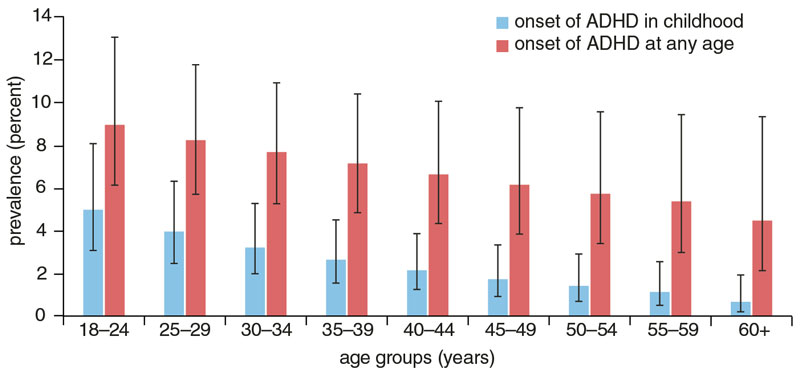
Let’s examine the possibility of an adult ADHD epidemic. This option would be possible only if adult-onset ADHD were a valid phenomenon. ADHD is classified as a neurodevelopmental disorder in the Diagnostic and Statistical Manual of Mental Disorders (DSM), a handbook published by the American Psychiatric Association to govern responsible diagnoses of mental disorders by health care practitioners. The neurodevelopmental disorder category (which also includes intellectual disability and autism spectrum disorder) is characterized by disrupted brain functioning stemming from abnormal neural development. ADHD is largely inherited through a person’s genes, but it is also influenced by environmental factors such as stressors and protective supports. As the DSM defines neurodevelopmental disorders, onset is in childhood, but the course usually lasts a lifetime. In the case of ADHD, the DSM requires onset of at least some symptoms—difficulties in self-regulation such as attention problems, hyperactivity, mental restlessness, and impulsivity—by age 12.
Consistent with the DSM’s description, research suggests that ADHD is a chronic and lifelong experience for most with the diagnosis. Studies investigating the possibility of true adult-onset ADHD have largely come up empty-handed. So, what explains rising rates of adult ADHD in the United States over the past five years?
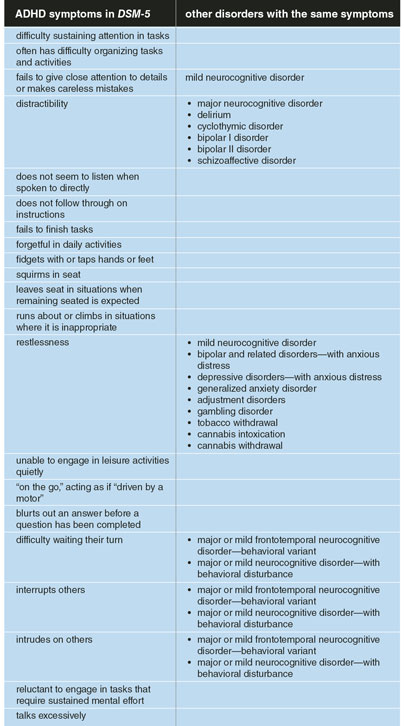
One factor may be that the DSM has become more inclusive. In 2013, the DSM was revised to its fifth edition with several changes that formally relaxed ADHD’s diagnostic criteria; however, it is unclear what effect these changes had on future diagnostic rates. DSM-5 pushed the cutoff for the age of onset from 7 to 12 years old, reduced the number of symptoms needed (from six to five) for an adult ADHD diagnosis, loosened the level of impairment (problems in daily life functioning) required for diagnosis, and allowed individuals with autism spectrum disorder to receive a co-occurring ADHD diagnosis. Ultimately, by expanding the diagnostic category, these changes may have increased rates of ADHD diagnoses in adults and children. The DSM revision happened in 2013, so it seems unlikely to have triggered the sudden spike in adult ADHD diagnoses in the 2020s. Still, relaxing the adult ADHD criteria may have been one source of kindling for that later explosive trend.
Illustration by Zachary Balcoff/The State News
Although the DSM-5 portrays ADHD as a disorder you either have or have not, that characterization is a false binary. Indeed, the diagnosis of ADHD demonstrates a condition that represents the extreme end of a trait continuum, similar to the range of severity in conditions such as hypertension and obesity.
Health care providers often use a checklist of behaviors which, in aggregate, form a person’s level of trait ADHD. Everyone falls somewhere on this continuum, which includes a person’s abilities in areas such as paying attention, organizing tasks, remembering daily activities, and modulating their verbal and motor activity levels. People with very low trait ADHD do very well with most of the behaviors on the checklist. People with high trait ADHD will struggle with many of them. If a person describes above average ability on the checklist, we call it a strength. When someone has below average ability, we call it a weakness or a symptom.
Trait ADHD displays a bell curve in the U.S. population, and providers must decide where to draw the line between weakness and clinical diagnosis. Formally, the DSM-5 offers a symptom cutoff for adults—at least five of nine formal symptoms of either inattention or hyperactivity/impulsivity. But ADHD symptoms are common and relatable—in fact, the average U.S. adult experiences two to three. How severe of an impairment is enough to deem a symptom as present? Conventional clinical wisdom advises that when a person can’t manage everyday life because of prominent and chronic ADHD symptoms, an ADHD diagnosis is appropriate. Yet, inevitably, clinicians encounter a gray area when individuals present with mild ADHD weaknesses and no obvious struggles in daily functioning.
Making an adult ADHD diagnosis can be done with confidence in someone like Jake, a 26-year-old I first met when he was a visibly hyperactive third grader. (Names and key identifying details have been changed throughout this article to protect patient confidentiality.) If Jake walked into a mental health clinic seeking evaluation for adult ADHD, he could share clear stories from his childhood as an athletic but severely bullied child who received help at school due to disabling problems focusing and completing schoolwork. His highly invested parents could corroborate Jake’s account with their own struggles wrestling with him over personal hygiene and sacrificing their free time to provide Jake the academic support needed to cross the high school finish line. Now in his mid-20s and still living at home, he appears friendless, withdrawn, and immersed in video games. Although it took him six years, he completed a bachelor’s degree in education, hoping to become a teacher. But with inconsistent motivation to engage in an employment search and challenges with social interactions, he has been working at the local zoo’s ticket counter. Since Jake does not have a car (he crashed the last two and could not afford a new one), his father drops him off each morning on his way to work.
Jake’s impairments due to his ADHD would be obvious to a clinician. He has experienced many negative consequences because of chronic, elevated trait ADHD, and these consequences reduce and interfere with his daily life functioning. Like Jake, adults with ADHD experience a range of consequences that can include employment instability, educational under-attainment, strained relationships with family members, limited social relationships, driving and safety incidents, and challenges managing a household. They also can experience hidden psychological impairments with self-esteem, stress response, anxiety, self-doubt, and feeling disconnected from others.
Compared with the general population, adults with subclinical ADHD are at elevated risk for secondary complications from their symptoms, such as substance use disorders.
Increasingly, health care providers are meeting with patients who experience a lighter form of ADHD. When Rebecca walked into a clinic for a possible first-time ADHD diagnosis, she was 41 years old. It had not occurred to her that she might have ADHD until Facebook ads started popping up on her feed during the COVID-19 pandemic. One said: “Working hard but not moving up? You might have undiagnosed ADHD.” Another said: “Indecisive? Anxious? A two-minute quiz can tell you if you have ADHD.” One day, her curiosity got the better of her, and she clicked on an image. Looking back on the past 20-plus years of her adult life, she wondered whether a diagnosis of ADHD would explain some of the struggles and disappointments she had experienced.
Most notable to Rebecca was her lack of success in the dating department. Sure, she had a serious boyfriend of four years who was a great, laid-back guy. He owned the house they lived in together and had a successful job. He was eight years younger and, like her, saw the prospect of children as a ball and chain to be avoided. Prior to this relationship, though, she had been devastated by two broken-off engagements and one long-term partnership in which she had been cheated on for years. Her entire social circle had known it was happening, but no one had said anything. Rebecca processed these experiences as personal failures that were her fault, though she could not quite explain what she had done wrong. She had many close friends and was gifted at several hobbies, including surfing and pottery—her pieces showed in local galleries and were a dependable income source. Nonetheless, Rebecca felt that she was not the full package.
It was not just intimate relationships that had been a source of emotional pain for Rebecca. Although she had graduated with honors from a top-notch college studying industrial design, she had bounced between jobs over the years, chronically indecisive about whether she preferred to work for herself or someone else. As a talented jack-of-all-trades, she could easily pick up work in several different arenas, but ultimately found these endeavors curtailed by the temptation to take off to work and travel abroad for months. Now, in midlife, she was questioning the life decisions that had left her living paycheck to paycheck, with no savings or assets.
Rebecca would be a much more challenging diagnostic scenario for clinicians than Jake. With no obvious childhood history of ADHD symptoms, some might dismiss the possibility of ADHD immediately. Yet Rebecca reports a moderate amount of relationship and employment instability, as well as financial impacts of her life decisions, paired with persistent feelings of self-blame and self-doubt. These negative experiences can be linked to a pattern of restlessness (a form of mental hyperactivity) in her life, but she reports only three symptoms of inattention and two symptoms of hyperactivity or impulsivity on an ADHD checklist—not enough for a diagnosis. Rebecca’s clinician might feel stuck on whether to make this borderline diagnosis of ADHD. Yet, after performing the due diligence of interviewing her boyfriend, Rebecca’s clinician becomes a bit more confident. Her boyfriend describes forgetfulness, difficulties with follow-through on household tasks, talkativeness, and distractibility as just “a part of who she is.”
Ultimately, the clinician evaluating Rebecca returns to the question of whether her symptoms are interfering with her functioning and decides to make the diagnosis. But, just as easily, another clinician might have dismissed Rebecca’s “ADHD-light” as subclinical (not severe enough for diagnosis), noting that the symptoms are not substantially interfering with her daily life and that her childhood history of ADHD is inconclusive.
Many, like Rebecca, sit in a gray area of the ADHD bell curve.
Before dismissing Rebecca’s ADHD entirely, let’s consider the defensible argument for treating adults with light or subclinical ADHD. Many subclinical adults go on to experience full ADHD at another point in their lives—so helping Rebecca now (with an evidence-based approach such as cognitive behavioral therapy or a low dose of medication) could be viewed as a form of prevention.
S. V. Faraone, et al. 2024.
Research suggests that subclinical ADHD is not always associated with ADHD’s signature cognitive differences such as executive function difficulties, and it is less likely to be associated with a family history of the disorder. Individuals with subclinical ADHD often do not experience meaningful impairments or co-occurring diagnoses and are more likely to notice benefits such as creativity from their ADHD than people with moderate to severe ADHD. Yet, compared with the general population, they are at elevated risk for secondary complications from their ADHD symptoms, such as substance use disorders. They also appear to respond to treatment in similar ways to individuals meeting full ADHD criteria. So, if Rebecca’s provider thought she could benefit from treatment, they might make the diagnosis to qualify her for care.
One factor that may be nudging subthreshold and mild ADHD patients such as Rebecca into clinics is the emerging neurodiversity movement. Diagnosed with ADHD, Rebecca feels she is seeing her life clearly for the first time and experiences meaningful relief with treatment. This transformational experience, felt by many late-diagnosed ADHD-light adults, is calling into question the rigidity of ADHD’s diagnostic requirements. The argument is that people like Rebecca—who might not meet ADHD’s traditional impairment and childhood-onset criteria—should not be denied the opportunity to hold a diagnosis that feels true to their identity and resonates with their lived experiences. This framing is part and parcel of the neurodiversity movement, whose ideas caught fire in the ADHD community during the COVID-19 pandemic. The neurodiversity framework encourages a more inclusive definition of adult ADHD as a fundamentally disabling neurotype, regardless of one’s external impairment level.
A clinician adhering to the neurodiversity conceptualization of ADHD might consider the concepts of masking (camouflaging ADHD symptoms to assimilate to social norms) and compensating (employing strategies that mitigate the impact of symptoms on daily life) when forming diagnostic conclusions. Ultimately, the clinician might override the need to demonstrate objective impairment or childhood symptoms if they can point to identifiable masking or compensatory factors that prevented the emergence of those symptoms. The neurodiversity movement also raises questions about whether the exhaustion from constantly suppressing one’s ADHD can supplant the impairment criterion. Interestingly, many common mental disorders in the DSM-5 have a “distress and/or impairment” criterion for establishing clinically sufficient severity, but ADHD employs only an impairment criterion.
Rebecca’s clinician might point to her intelligence and sought-after talents as strengths that masked her childhood symptoms and allowed her to compensate for ADHD as an adult. If she had not been so good at school and so charismatic in her personality, perhaps ADHD traits would have visibly emerged in childhood. If she had not had multiple monetizable skills, and a boyfriend providing free housing, her prominent restlessness could have become a serious threat to her financial survival. Even Jake found ways to offset his ADHD with help from his parents—what would his life be like today if they had not pushed him through his education, given him a stable place to live, and provided him with reliable transportation? Still, if a person is a sum of their parts, then it’s also defensible to take a holistic view of ADHD—that Rebecca is a person whose net impairment level is not that meaningful.
The transformational experience felt by many late-diagnosed “ADHD-light” adults is calling into question the rigidity of ADHD’s diagnostic requirements.
Several pandemic-related factors may have also contributed to the tug-of-war over ADHD’s diagnostic borders. As people began to spend more time online during lockdowns, many people increasingly shared their diverse lived experiences with ADHD. An explosion of ADHD anecdotes shared on social media may or may not have aligned with scientifically validated information about the disorder, but they certainly stretched the public’s conceptualization of ADHD’s many faces. Because novel rather than tried-and-true information garners the most social media clicks, a long list of “secret” or “unrecognized” crowdsourced ADHD symptoms began to proliferate online. As this list grew, so did the number of people who found the ADHD diagnosis to be relatable.
The rise of the #ADHD world also created some moneymaking opportunities. Many ADHD posts touting lived experience linked directly to purchasable products or services such as supplements or coaching. Most notably, several large-scale digital start-ups seized an opportunity in the midst of relaxed U.S. laws for prescribing stimulants (the main class of medications for ADHD) and began offering quick and easy online diagnoses to support their economy-of-scale business models. They unleashed a sea of digital ads upon their potential consumers (such as the post that caught Rebecca’s eye). These ads also may have influenced self-referral rates for ADHD—through a digital start-up or otherwise. It is worth noting that a few ADHD-centric prescribing companies (such as Cerebral and Done) later fell under federal investigation for predatory practices and subsequently folded their controlled-substance–prescribing operations. At the very least, we can say that the internet had developed a vested interest in expanding the definition of who could benefit from ADHD-related products and services.
A growing women’s movement within the ADHD community may also be increasing self-referrals for ADHD diagnoses. As the CDC and other sources reveal, the majority of adults seeking diagnosis and treatment for the first time are women in their 20s, 30s, and 40s. The 2020s have witnessed a powerful great awakening of women who came to identify with the ADHD diagnosis for the first time by sharing lived experiences with one another online.
The surge among women makes sense. It is well established that ADHD has been diagnosed at lower rates in girls than in boys. Because research on ADHD has historically excluded girls, we do not fully know if this trend reflects a structural inequity, later onset of ADHD in girls and women (perhaps influenced by hormonal factors), or a lower prevalence of girls and women at the extreme end of the trait ADHD distribution (perhaps due to protective effects of being biologically female on the expression of ADHD genetic risks).
The ADHD women’s movement is mobilizing around the sentiment that women with ADHD were missed en masse during childhood due to diagnostic criteria that favor men and boys.
In a grassroots fashion, the ADHD women’s movement is mobilizing around the sentiment that women with ADHD were missed en masse during childhood due to diagnostic criteria that favor men and boys. One action item of this ADHD advocacy space is a push to expand the DSM-5 criteria to better address the clinical presentations of women with ADHD. The diagnostic implications of the ADHD women’s movement are complex, and women are indisputably expanding definitions of what ADHD can look like. However, research has not yet sorted out best practices for identifying ADHD in girls and women.
ADHD’s recent surge, however, is probably not just a societal change in how we define and recognize the disorder. Emerging research has revealed that, within an individual, ADHD can be highly unstable across the lifespan. Thus it’s possible that more Americans are experiencing clinically meaningful difficulties with ADHD since the pandemic. Many, if not most, individuals with ADHD will meet formal diagnostic criteria for the disorder during some years but not others. Some research confirms that fluctuations in environmental demands can influence the ups and downs of an individual’s ADHD. What’s more, ADHD symptoms can wax and wane even in people without ADHD.
This way of thinking lines up with the idea that genes and environment work together in ADHD. In other words, whether someone’s genetic risk for ADHD shows up in real life can depend on what’s happening around them. So, if certain things in society made ADHD symptoms worse, people who were already on the edge of having ADHD might have started feeling a lot more symptoms all at once—and many may have looked for some kind of support at the same time, whether that meant medication, therapy, coaching, or even supplements.
This idea matches what psychologists Maria A. Rogers of Carleton University in Ottawa, Canada, and Jaidon MacLean of the University of Ottawa found in their 2023 meta-analysis: Around the world, ADHD symptoms went up during the pandemic. So, if ADHD symptoms got worse during the pandemic, and if people started talking about ADHD more openly on social media, it makes sense that in the early 2020s more people like Rebecca—who would traditionally fall into the gray, subclinical area—started wondering if they had ADHD. But what caused the jump in official diagnoses? One likely reason is the rise of easy-to-access telehealth services, such as those offered by online mental health companies. According to a 2024 CDC report, about one in five adults with ADHD got their diagnosis using online modalities, and half have used telehealth for ADHD care in the past few years.
What is a clinician to do? If an individual who normally has subclinical ADHD visits a clinic during a period when their symptoms spike into the clinical zone, should a practitioner provide a diagnosis of ADHD? Doing so is probably not overdiagnosis since the individual will likely meet all criteria for ADHD (DSM-5 requires several symptoms to be present since childhood, not the full syndrome). In future years, the broader field will likely recognize ADHD’s fluctuating course across the lifespan and the factors that trigger ADHD flare-ups. The ADHD diagnosis will inevitably become more inclusive as the science of ADHD’s fluctuations translates into clinical practice.
Adults who recognize themselves in the expanding list of relatable, crowdsourced ADHD symptoms may be self-diagnosing or wondering about possible ADHD, and some may have raised this possibility with their health care providers. It is not clear whether adoption of the neurodiversity framework is as widespread among clinicians as it is on social media. However, there is certainly a growing tension between traditional and alternative ways of thinking about ADHD diagnosis within the clinician workforce. The supposition that clinicians must wade through a pit of what-ifs to unearth a largely unimpaired individual’s true ADHD neurotype is a tall order for many. Although an individual’s level of trait ADHD correlates highly with their genetic load for the disorder, there is no definitive biomarker for ADHD. Some people with elevated genetic risk of ADHD do not display the disorder. Other people with ADHD do not demonstrate a strong genetic load. Trait ADHD is influenced by an interplay of complex biological, psychological, and environmental factors.
V. Karasavva, et al. 2025.
To complicate matters, ADHD is best conceptualized as a bundle of cognitive subtraits (such as working memory, response to rewards, and the ability to inhibit one’s behavior) that contribute to an overarching ADHD behavioral trait. People who achieve a high score on an overall trait ADHD behavioral checklist will show widely varying combinations of these cognitive subtraits. Thus, there are undoubtedly different neurobiological paths to ADHD, and the volume may be turned up or down on those paths based on a range of stable or transient factors. Since ADHD is such a neurocognitively diverse category, there is no objective cognitive test that can reliably confirm the diagnosis. Instead, we clinicians rely on documenting a stable, impairing pattern of observable behaviors consistent with ADHD that are substantiated by multiple individuals.
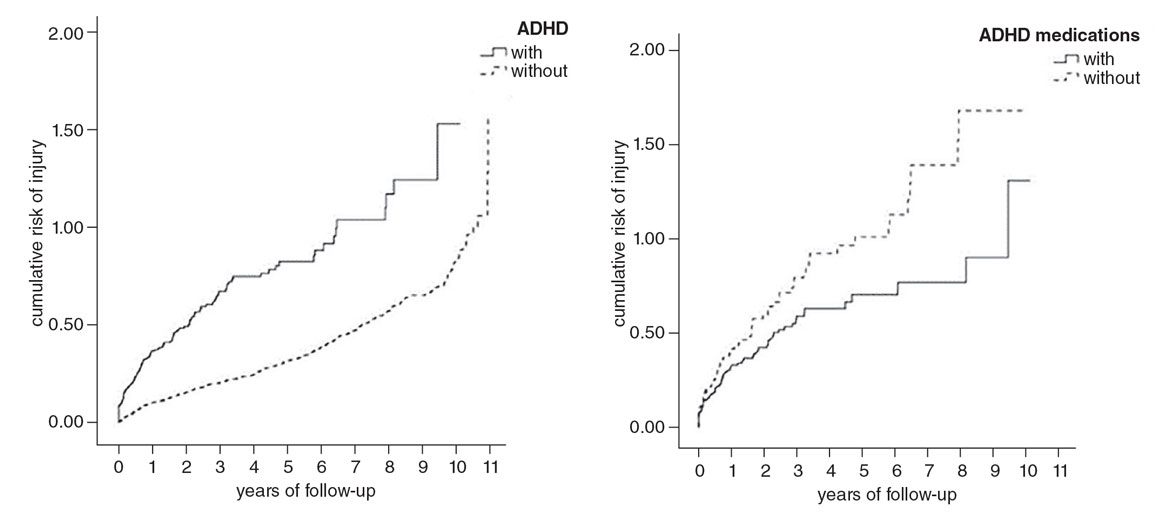
A. R. Kosheleff, et al. 2023; graphic reprinted with permission from W. C. Chien, et al. 2017. Research in Developmental Disabilities.
Right now, there are both vocal advocates and opponents of the neurodiversity framing of ADHD. I have also met open-minded clinicians who feel the neurodiversity framework makes a lot of sense but are hesitant to step away from upholding the strict impairment and childhood-onset criteria. They fear that the boundaries of ADHD will become far too subjective, which will bruise its credibility. They are very protective of a diagnosis that is clearly so disabling to those who meet its strict criteria.
ADHD has always experienced stigma from skeptics in the public and in the broader medical field. For various reasons, similar scrutiny has not been passed on to sister diagnoses such as autism spectrum disorder or learning disorder, or to spectrum-based medical diagnoses such as hypertension or diabetes. Since ADHD traits are on a continuum and can show up in the general population, the impairment and childhood-onset criteria have acted as important checks and balances. The diagnostic line will inevitably become much blurrier if we kick them out of place.
Many individuals with ADHD will meet formal diagnostic criteria for the disorder during some years but not others. What’s more, ADHD symptoms can wax and wane even in people without ADHD.
ADHD is already vulnerable to misdiagnosis, and so affixing an overdiagnosis narrative has been tempting to those outside the ADHD community. As a standard part of the adult ADHD diagnostic assessment, clinicians must wade through a complicated process of ruling out other disorders with overlapping symptoms. There are many non-ADHD-related factors that alter the neurochemical environment of brain structures implicated in ADHD. For example, psychiatric disorders such as anxiety and depression, side-effects of medications taken for reasons unrelated to ADHD, normal responses to stress or poor sleep, endocrine disorders, and transitions such as hypothyroidism or perimenopause can all cause ADHD-like symptoms. Differential diagnosis is often the most time-consuming part of a properly performed adult ADHD evaluation. Multiple, long encounters are sometimes needed to confidently complete this process. Modern health care systems cannot always accommodate this level of due diligence, which creates a vulnerability to misdiagnosis.
But for just as many occasions where ADHD is improperly diagnosed, it also is likely missed. Many late-identified adults with ADHD initially come into contact with the mental health system for co-occurring diagnoses such as anxiety, substance use disorders, or depression. Often, undiagnosed ADHD is at the root of these secondary complaints, but it is missed by the untrained eye. Thus, for every adult ADHD overdiagnosis there is likely an underdiagnosis.
Many late-identified adults with ADHD initially come into contact with the mental health system for co-occurring diagnoses. Often, undiagnosed ADHD is at the root of these secondary complaints.
The COVID-19 pandemic created global exacerbations in mental health concerns and a subsequent influx of people seeking help for ADHD and other psychiatric disorders. This unprecedented demand for mental health support required an expansion of the provider workforce, which shifted new providers into the task of making first-time adult ADHD diagnoses. It appears that many primary care doctors and nurse practitioners stepped up to meet this need (as did instant-diagnosis digital start-ups, some of which have been accused of predatory practices). Newer providers may be more vulnerable than a veteran ADHD specialist to confusing ADHD for a mimic; they may also be more open to inclusive viewpoints on the nature of ADHD in adults.
Scientists have long understood ADHD as a collection of related disorders that impact self-regulation, making it vulnerable to becoming a catch-all category for anyone with attentional concerns. This diagnostic lumping may be expanding the inclusiveness of the ADHD category and producing diagnostic rates that cause public discomfort. Partitioning rather than discrediting ADHD may be a consideration. For example, over the past 75 years the DSM has partitioned the previously singular diagnosis of depression into separate categories that include major depressive disorder, persistent depressive disorder, disruptive mood dysregulation disorder, and premenstrual dysphoric disorder. Perhaps it is time to do the same with ADHD.
Adapted from M. K. Forbes, et al. 2023.
The process of subdividing ADHD into a broader class of multiple disorders must be done through careful research that examines the full implications of diagnostic changes. The vocabulary surrounding future changes is also important. As with depressive diagnoses, reorganization of a broader category of disorders of attention and self-regulation might consider severity (is there a lighter form of ADHD that mainly impacts psychological factors?), course (are there female sex–specific versions of ADHD with pubertal or perimenopausal onsets?), persistence and stability (is there ADHD that fluctuates with environmental factors?), and features (is there a form of ADHD that is largely experienced as emotional dysregulation?).
The critical point is that everyone’s experience of ADHD-like difficulties, and their impacts on how one walks through life, are valid. Our diagnostic categories need to do a better job of capturing the many faces of ADHD and of helping patients and clinicians see eye to eye on diagnostic conclusions. Until diverse disorders of attention and self-regulation are properly sorted, ADHD will continue to become more and more inclusive as additional forms of self-regulation concerns are recognized and pushed into the only diagnostic category available to them. Despite the many reasons why diagnostic lumping is problematic, people like Jake and Rebecca still need help, and we want to make sure they can get it.
This essay is adapted from a version published on Aeon.
Click "American Scientist" to access home page

American Scientist Comments and Discussion
To discuss our articles or comment on them, please share them and tag American Scientist on social media platforms. Here are links to our profiles on Twitter, Facebook, and LinkedIn.
If we re-share your post, we will moderate comments/discussion following our comments policy.