Physicians Need Caregiving Support Policies
By Katie L. Burke
The collision of the Great Resignation and long-standing gender inequities in medicine is heightening calls for improved family leave policies at American health care institutions.
The collision of the Great Resignation and long-standing gender inequities in medicine is heightening calls for improved family leave policies at American health care institutions.

Even before the COVID-19 pandemic hit in 2020, rates of promotion and retention for women physicians were known to fall far short of gender parity. Although just over 50 percent of medical students are women, only 37 percent of practicing doctors are women. A 2020 report by the Association of American Medical Colleges shows that representation of women in academic medicine declines as one climbs the promotional ladder (see the figure below). One 2019 study showed that nearly 40 percent of women physicians left the career or cut back their hours within six years of finishing their residencies. Moreover, a 2022 JAMA Network Open study showed that little progress had been made between 1990 and 2019 to increase the number of women faculty of color in academic medicine, despite some progress among white women. Research has repeatedly shown that women in medicine report higher rates of burnout and depression than men do, and they cite home responsibilities as primary reasons for leaving their jobs, cutting back hours, or missing out on promotions.
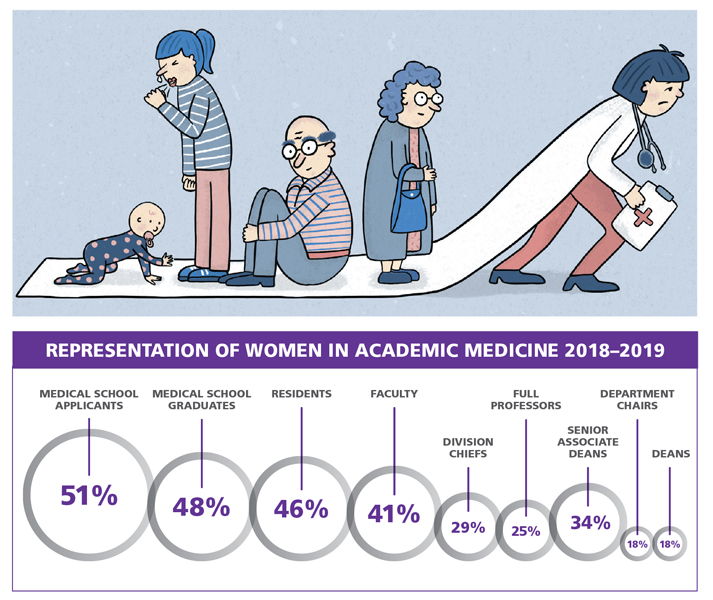
Cartoon by Hannah Wirenfeldt Moore/Northeastern University; Courtesy of Association of American Medical Colleges
Managing the stressors associated with the pandemic—including caregiving needs at home and strained health care and childcare systems—disproportionately fell to women, especially those of color. Comprehensive data are not yet available, but a December 2021 survey of 9,266 physicians at 124 U.S. institutions found that 1 in 5 physicians planned to leave their practices within two years. Given that women are already more likely to leave the field, this information points to a looming postpandemic spike in attrition among women physicians. “We’re facing an existential threat in academic medicine,” says Christina Mangurian, a psychiatrist, an expert on caregiving support policies, and the vice dean for faculty and academic affairs at the University of California, San Francisco, School of Medicine. “We could lose a ton of women right now.”
Supportive family leave and childcare policies are an effective way for institutions to make a big difference in retention. The amount of support a physician has varies substantially by state and institution. “Evidence from the business world shows that generous parental leave and caregiving policies lead to workers who feel more connected to the organization and are less likely to leave,” says Neda Laiteerapong, an associate professor of medicine at the University of Chicago. “But academic medical schools are not at the forefront on this issue.” Such policies have known and established benefits. “Limited paid parental leave policies have been shown to increase rates of burnout, increase rates of mental health problems, and lower rates of breastfeeding,” Laiteerapong says. Faced with a workplace that asks them to take on more work, but advances them less, many women decide to leave.
When women physicians leave their careers, all sorts of problems compound: Many health care institutions cannot afford to lose part of their labor pool, and the remaining workforces do not reflect the populations that they serve. As a physician shortage looms, calls for implementing policies that support equity at the institutional, state, and national levels have taken on a sense of urgency. (See “Balancing Home and School,” November–December 2022.)
Despite the clear need—and despite abundant evidence of the benefits of paid leave for workers and patients alike—research shows that medical employers generally do not have adequate family leave policies. A study published in January in JAMA Network Open and led by Laiteerapong found that only 15 percent of medical schools offered their faculty 12 weeks of paid parental leave. Forty percent had no adoption paid leave policy at all, and 75 percent had no foster paid leave policy. Due to the early-career demands of the profession, many physicians need policies that support the unique challenges of in vitro fertilization, adoption, or foster parenting. The study also showed that highly ranked and well-funded institutions tend to offer the most supportive policies. “Very few physicians practice at the top institutions,” Laiteerapong says, pointing out that most physicians are left out of the group with flagship policies.
Only 15 percent of medical schools offered their faculty 12 weeks of paid parental leave.
“The majority of workers in this country are family caregivers at some point in their career,” says Jessica Lee, director of the Pregnant Scholar Initiative at the Center for WorkLife Law, based at the University of California, San Francisco (UCSF). “Yet the STEM education career pathway was designed for folks who weren’t managing family care.” Even when policies appear to be in place, the details and wording can block access to them. “[STEM professionals] keep hitting a brick wall of bureaucracy,” Lee says. “It’s infuriating and heartbreaking to see these generations of brilliant minds thrown off track, completely needlessly.”
About 16 percent of physician mothers in the United States are informal caregivers for parents or children, according to a 2019 study led by Mangurian. She has assessed policies that support caregivers in medicine at all career levels. The focus for supporting caregivers has largely been on new parents, but Mangurian found that more of the faculty doing informal caregiving at her institution were caring for their elderly parents than young children, pointing to the need for policies that take into account all forms of caregiving.
Changes are happening at the national, state, and institutional level, although most existing policies still fall short of the support caregivers need. In March, the U.S. Commerce Department announced that tech companies seeking federal funding through the CHIPS and Science Act, a law passed last year that provides about $280 billion of funding for domestic research and manufacturing of semiconductors, will be required to provide childcare for their workers. An increasing number of states are creating parental and family leave standards that are more generous than those set at the national level by the U.S. Family and Medical Leave Act, which requires employers of a certain size to offer 12 weeks of unpaid leave—one of the least generous parental leave policies among developed countries. In 2022, Maryland, Virginia, and Delaware all updated their parental and family leave policies, with Maryland and Delaware requiring 12 weeks of paid leave. At the institutional level, medical professionals are seeing more policies that recognize the importance of supporting employees that have caregiving responsibilities at home.
Even when leave and childcare policies are in place, there are barriers to accessing them. For example, in many cases in which daycare is available through an employer, waitlists are often so long that in order to guarantee a spot, parents need to get on the list before they even know whether they will have a baby to enroll. Lee points out that having a family leave or childcare policy on paper doesn’t always mean every employee can access that support.
The problem pervades all levels of the medical profession. There is no standardized, standalone parental leave policy for medical students. For residents, the Accreditation Council for Graduate Medical Education (ACGME) last year raised their standard to six weeks of paid leave, which is progress but still far shorter than the 12 weeks recommended by the American Academy of Pediatrics or the paid leave offered in other developed countries.
Some specializations are shockingly out of step with contemporary workplace culture. Lee coauthored a study published in the Journal of the American College of Cardiology last year that surveyed 323 women in the profession about their experiences with childbearing and parental leave. She and her coauthors found that pregnant cardiologists generally are expected to make up their time away from work before they go on leave. “Cardiologists were not getting the maternity leave that they are legally entitled to,” Lee says. “And they were facing pay cuts when they came back from maternity leave, regardless of whether they preworked those hours or not. Then, after they gave birth they were still asked to work while on maternity leave.” Cardiologists who put in extra clinic service and call time before their family leave were more likely to experience pregnancy complications such as bedrest. “They were working themselves sick at tremendous personal costs, without even realizing that what they were being asked to do is illegal,” Lee says.
Because these workplace expectations were not formalized, they were legally flying under the radar, even though they were clearly having a discriminatory effect—only 14.9 percent of practicing cardiologists in 2020 identified as women. Lee emphasizes that working people struggling with issues around childbearing and family leave must push back against unsupportive workplace norms. Resources such as ThePregnantScholar.org and the free legal help line at the Center for WorkLife Law are there to assist workers struggling with questions about balancing employment with childbearing or caregiving.
In the void left by a lack of a national or state policy, changes can be made at the institutional level. Organizations that enforce standards in the field, such as ACGME and funding agencies, can make a big difference, as can individual institutions. In 2019, Mangurian worked with the leadership at the UCSF School of Medicine to change the family leave policy for UCSF medical faculty. UCSF now has 12 weeks of paid leave, regardless of adoption or birth and regardless of the parents’ gender or sexual orientation. Ultimately, though, national policies will be the most effective way of ensuring that all workers with caregiving responsibilities at home are able to continue their careers.
Click "American Scientist" to access home page

American Scientist Comments and Discussion
To discuss our articles or comment on them, please share them and tag American Scientist on social media platforms. Here are links to our profiles on Twitter, Facebook, and LinkedIn.
If we re-share your post, we will moderate comments/discussion following our comments policy.